Ear Hematoma – Treatment
Ears, Eyes, Nose, and Throat
Context
Ear (auricular) hematoma, is the collection of blood between the perichondrium and underlying cartilage within the cartilaginous auricle (pinna), typically resulting from blunt trauma.
- Classically presents as a tender, tense, fluctuant collection of blood on the anterior aspect of the pinna (Figure 1).
- Overlying skin can be erythematous or ecchymotic
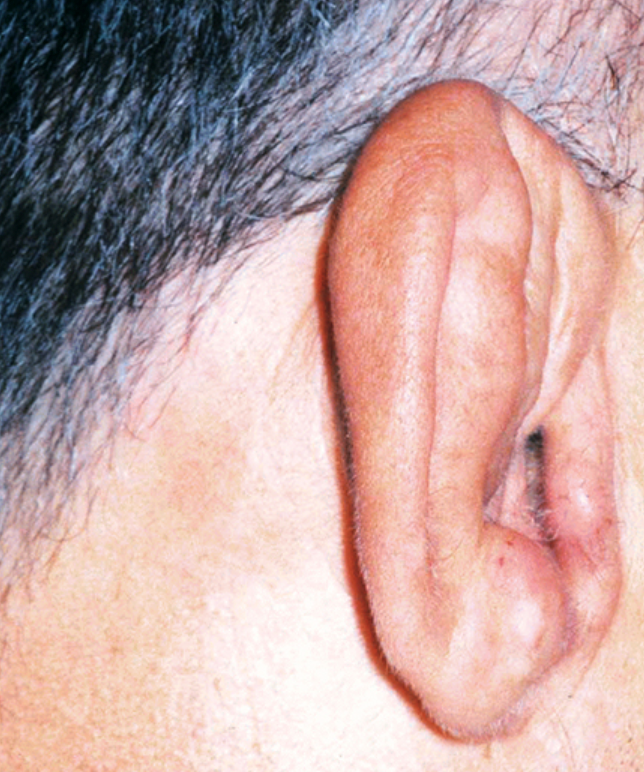
“Cauliflower ear” is the permanent deformity caused by fibrocartilage overgrowth that occurs when an auricular hematoma is not fully drained, recurs, or is left untreated.
- Classically, is presented as a bulbous deformity of the pinna (Figure 2).
Pathophysiology
- Underlying cartilage necroses due to lack of perfusion, resulting in cartilage loss, fibrosis, and neocartilage formation.
- Early identification and drainage of hematoma, and restoration of cartilage perfusion are important to prevent the permanent formation of cauliflower ear.
Risk factors:
- Trauma from sports injuries (e.g. wrestling, rugby, boxing, or mixed martial arts).
- Trauma in individuals who are anticoagulated.
Evaluation
- If significant trauma has occurred it is important to evaluate the middle or inner ear structures: CT should be considered.

Recommended Treatment
Drainage includes
- Needle aspiration.
- Incision and drainage, or intravascular catheter.
- After drainage, horizontal or vertical mattress stitches may be applied to effectively reduce the dead space and to prevent re-accumulation of blood or fluid (see Figure 3.).
- Patients who opt for no treatment accept poor cosmetic outcomes.

Needle Aspiration
- Cleanse the ear with antiseptic and provide local anesthesia.
- Use an 18 gauge needle to aspirate the most fluctuant part of the hematoma. Milk the hematoma to ensure complete drainage.
- Apply pressure for 5 to 10 minutes after needle aspiration.
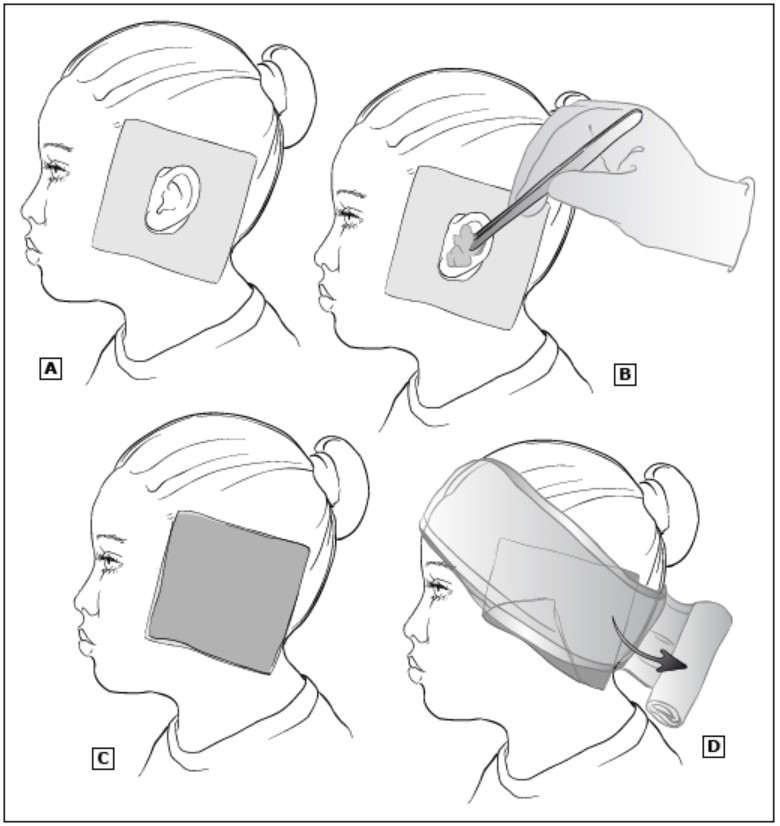
- Apply a pressure dressing (see Figure 4.)
- Place sterile gauze with a central cut out to provide padding behind the ear.
- Mold petrolatum-impregnated gauze or saline-soaked cotton balls within the contours of the auricle. If the skin was incised, this portion of the dressing needs to reapproximate the skin at the incision site.
- Place sterile gauze over the entire ear.
- Wrap the ear and head with sterile, rolled gauze to hold the dressing in place.
Incision and drainage
- Cleanse the ear with antiseptic and provide local anesthetic infiltration using buffered lidocaine without epinephrine. Epinephrine should be avoided to prevent disruption of vascular supply to ear cartilage.
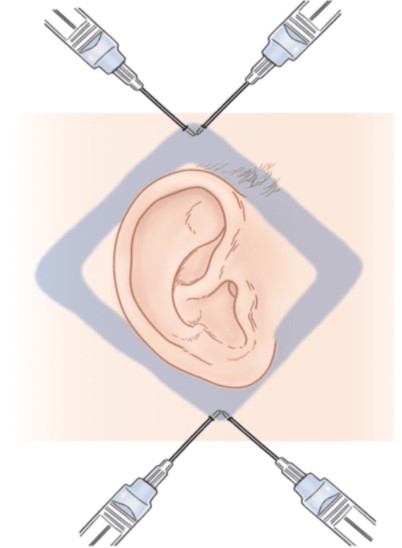
- A regional auricular block is indicated for the repair of extensive auricular lacerations or to avoid local tissue distortion when cosmetic alignment is important (see Figure 5.)
- Cleanse ear with an antiseptic solution such as providone-iodine solution.
- Inject buffered lidocaine 1% with epinephrine using a long, small gauge (25 or 27 gauge) needle. The total dose of lidocaine administered should not exceed 7mg/kg of lidocaine 1% (1%-10mg/ml).
- Enter the skin just below the ear and advance the needle posteriorly along the skin over the mastoid behind the ear.
- Inject up to 5mL of lidocaine as the needle is withdrawn. Without removing the needle, redirect the needle anterior to the ea and inject up to 5mL of lidocaine again. The tracks should form a “V”.
- Enter the skin just above the ear and advance the needle posteriorly behind the ear and inject up to 5mL of lidocaine. Without removing the needle, redirect the needle anterior to the ear and inject up to 5mL of lidocaine again. The tracks should form an inverted “V”. Wait 10 minutes.
- Use a 15 or 11 blade to make an incision along the curvature of the auricle at the base of the hematoma. The incision should be adequate to drain clotted blood.
- Irrigate the pocket with sterile saline.
- Suture the incision closed with mattress stitches or a bolster.
Intravenous catheter evacuation
- Cleanse ear with antiseptic and provide local anesthesia.
- Insert an 18 gauge intravenous catheter along the inferior border of the hematoma, attach as a syringe, and evacuate.
- Remove the needle but leave the catheter in position.
- Clip the catheter so that approximately 1cm protrudes from the insertion site to allow further drainage and apply gauze and elastic bandage.
Criteria For Hospital Admission
- Associated trauma or infection.
- Ongoing bleeding.
Criteria For Safe Discharge Home
- Pain managed.
- Follow-up is recommended with otolaryngology or plastic surgery. All patients should be re-evaluated every 24 hours for 3 to 5 days.
- Avoid aspirin and other NSAIDs.
- Patient should limit physical activity for 10 to 14 days and avoid contact sports for 1 to 2 weeks.
- If a splint is used, this will need to be removed in 5 to 7 days.
Criteria For Close Observation And/or Consult
- Appropriate consults and referrals for auricular hematoma are otolaryngology or plastic surgery.
- If concern for associated external, middle, or inner ear pathology, consult ENT.
Related Information
Reference List
Relevant Resources
RESOURCE AUTHOR(S)

DISCLAIMER
The purpose of this document is to provide health care professionals with key facts and recommendations for the diagnosis and treatment of patients in the emergency department. This summary was produced by Emergency Care BC (formerly the BC Emergency Medicine Network) and uses the best available knowledge at the time of publication. However, healthcare professionals should continue to use their own judgment and take into consideration context, resources and other relevant factors. Emergency Care BC is not liable for any damages, claims, liabilities, costs or obligations arising from the use of this document including loss or damages arising from any claims made by a third party. Emergency Care BC also assumes no responsibility or liability for changes made to this document without its consent.
Last Updated May 03, 2021
Visit our website at https://emergencycarebc.ca
COMMENTS (0)
Add public comment…
POST COMMENT
We welcome your contribution! If you are a member, log in here. If not, you can still submit a comment but we just need some information.