Dementia – Diagnosis
Neurological, Psychiatric and Behaviour
Context
- Dementia patients have higher emergency department (ED) utilization and hospitalization rates compared to patients who do not have dementia.
- Dementia continues to be underrecognized in older ED patients and should be screened for.
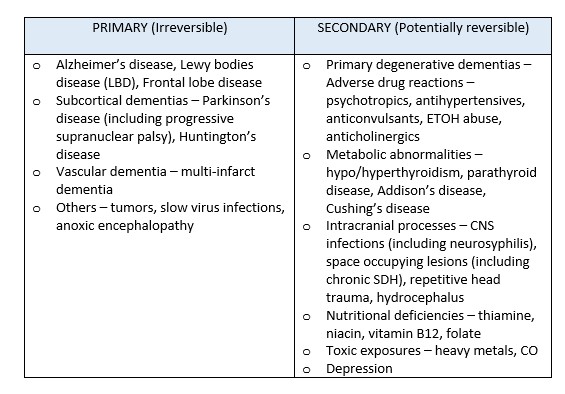
- Dementia is a chronic, clinical syndrome that is marked by gradual, progressive cognitive decline classified as either primary degenerative (irreversible) or secondary (potentially reversible).
Causes of Dementia
- Often present due to an acute deterioration in mental status or behavioural change such as refusal to eat. Often it is the caregivers who identify the change.
- Primary goal is to recognize the clinical presentation of undiagnosed and potentially reversible forms of dementia.
- Admission criteria for patients with dementia are influenced by the fact that they often have difficulty adapting to changes in environment if admitted to hospital.
- Following a person-centred approach helps to destigmatize dementia.
Diagnostic Process
- Dementia is a clinical diagnosis requiring a full workup that can be started in the ED.
- complete history, physical examination, associated cognitive screening, and laboratory investigations to rule out any underlying reversible causes.
- Physical examination should include a neurologic examination and evaluation of mental status.
- Patients with dementia will often exhibit confusion, but unlike delirium, will have minimal to absent autonomic nervous system abnormalities (i.e. stable vital signs) and normal level of consciousness (i.e. intact attention).
- Standardized tools can be used in the ED to quickly assess mental status and check for cognitive dysfunction:
- Mini-Mental State Examination (MMSE)
- Clock drawing test,
- Orientation-Memory-Concentration test,
- Abbreviated Mental Test (AMT-4),
- Brief Alzheimer’s Screen
- Meta-analyses have shown that the AMT-4 is currently the most accurate ED screening tool for ruling in dementia and the Brief Alzheimer’s Screen most accurate for ruling out.
- Diagnostic criteria for dementia (major neurocognitive disorder), according to DSM-V:
- Evidence of cognitive decline from a previous level of performance in one or more of the following domains: complex attention, executive function, learning and memory (short-term and long-term), language, perceptual motor function, social cognition.
- The cognitive deficits interfere with independence in everyday activities.
- The deficits do not occur exclusively during the course of a delirium.
- The deficits are not better explained by any other mental disorder.
- Laboratory investigations including CBC, metabolic panel, thyroid studies, urinalysis, and a non-contrast head CT.
- Additional investigations such as MRI, LP with CSF analysis, serum B12 and folate levels, and urine screen for heavy metals guided by history and physical examination.
Clinical Pitfalls
- Failure to screen for delirium. Both affect cognition, but in different ways and over a different time course.
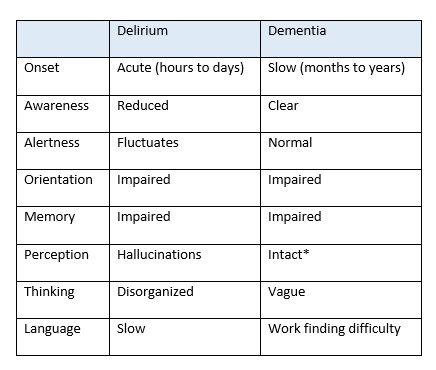
*LBD may have visual hallucinations
- Failure to recognize patients with some level of cognitive impairment in the ED who should still undergo further neuropsychiatric evaluation.
- Failure to assess a patient’s cognitive status and not do appropriate screening in the ED.
Recommended Treatment
- While the recognition and work-up are important and may be initiated in the ED, often a definitive diagnosis is made upon subsequent assessments.
- If there is no acute medical issue requiring admission or safety concern for discharge refer to an outpatient setting for follow-up.
- If there are no local options for outpatient follow-up, the Clinic for Alzheimer Disease and Related Disorders (CARD) at UBC Hospital is an alternative option.
Quality Of Evidence?

High
We are highly confident that the true effect lies close to that of the estimate of the effect. There is a wide range of studies included in the analyses with no major limitations, there is little variation between studies, and the summary estimate has a narrow confidence interval.
Moderate
We consider that the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. There are only a few studies and some have limitations but not major flaws, there are some variations between studies, or the confidence interval of the summary estimate is wide.
Low
When the true effect may be substantially different from the estimate of the effect. The studies have major flaws, there is important variations between studies, of the confidence interval of the summary estimate is very wide.
Justification
There is insufficient evidence to recommend a specific screening tool that is both sensitive and specific for detecting dementia in the emergency setting, and there are no specific ‘routine’ investigations recommended in the evaluation of suspected dementia.
Related Information
Reference List
Related Information
OTHER RELEVANT INFORMATION
Relevant Resources
RESOURCE AUTHOR(S)
DISCLAIMER
The purpose of this document is to provide health care professionals with key facts and recommendations for the diagnosis and treatment of patients in the emergency department. This summary was produced by Emergency Care BC (formerly the BC Emergency Medicine Network) and uses the best available knowledge at the time of publication. However, healthcare professionals should continue to use their own judgment and take into consideration context, resources and other relevant factors. Emergency Care BC is not liable for any damages, claims, liabilities, costs or obligations arising from the use of this document including loss or damages arising from any claims made by a third party. Emergency Care BC also assumes no responsibility or liability for changes made to this document without its consent.
Last Updated Jun 05, 2021
Visit our website at https://emergencycarebc.ca
COMMENTS (0)
Add public comment…
POST COMMENT
We welcome your contribution! If you are a member, log in here. If not, you can still submit a comment but we just need some information.