Priapism – Diagnosis
Urological
Context
- Priapism is a pathologic, prolonged penile erection without sexual stimulation, generally lasting longer than four hours.
- It can occur in males of any age, although it is rare in pediatrics. When present in the pediatric population, it is usually a complication of sickle cell disease.
- Priapism exists in two main forms: ischemic (low flow) and non-ischemic (high flow).
- Ischemic priapism results from failure of venous outflow from the penis and is a form of compartment syndrome—it is a urologic emergency requiring treatment in the emergency department and/or urgent urology consultation.
- Non-ischemic priapism results from increased blood flow through the corpora cavernosa with maintained venous outflow. It is typically a manifestation of an AV fistula formed from trauma or previous intervention for ischemic priapism. Flow is maintained, so it is not inherently dangerous. It can generally be managed as an outpatient.
- Stuttering priapism is a rare condition characterized by recurrent episodes of ischemic priapism and is often idiopathic.
- Short-term sequelae:
- Urinary retention.
- Penile thrombosis.
- Venous thromboembolism.
- Long-term sequelae:
- Erectile dysfunction.
- Transient or permanent changes in penile sensation.
- Development of penile curvature.
- The clinical starting point is diagnosis, and the clinical endpoint is discharge home with outpatient follow-up or urgent urology consultation +/- admission.
Diagnostic Process
- Diagnosis is generally clinical but if there is uncertainty, penile blood gas analysis can help to differentiate ischemic and non-ischemic priapism.
- Doppler ultrasonography may be used as an adjunct to the clinical evaluation, but it is generally not diagnostic.
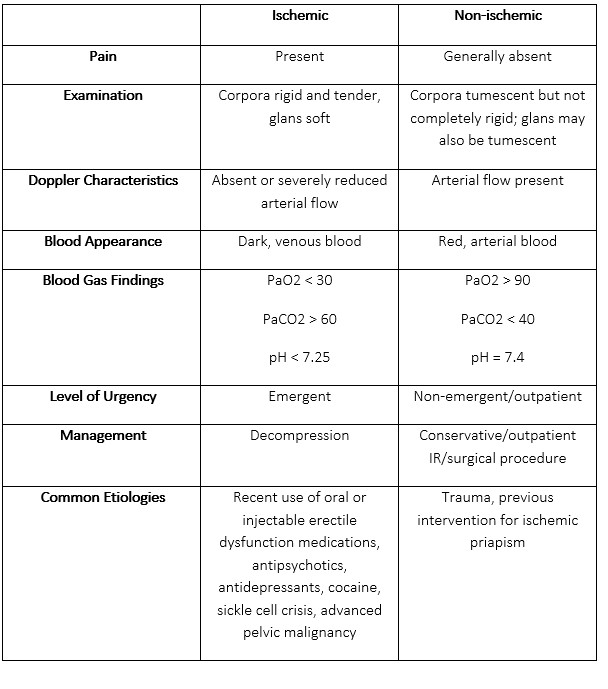
Table 1. Comparison of Ischemic and Non-ischemic Priapism
Quality Of Evidence?

High
We are highly confident that the true effect lies close to that of the estimate of the effect. There is a wide range of studies included in the analyses with no major limitations, there is little variation between studies, and the summary estimate has a narrow confidence interval.
Moderate
We consider that the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. There are only a few studies and some have limitations but not major flaws, there are some variations between studies, or the confidence interval of the summary estimate is wide.
Low
When the true effect may be substantially different from the estimate of the effect. The studies have major flaws, there is important variations between studies, of the confidence interval of the summary estimate is very wide.
Justification
This resource is based on moderate quality evidence from the emergency medicine literature, academic texts, and clinical resources. The diagnostic modality of choice to confirm ischemic priapism is arterial blood gas analysis. Doppler ultrasonography can be used as an adjunct but should not replace it.
Related Information
Reference List
Davis JE and Silverman MA. Urologic Procedures. In: Chanmugam AS, Chudnofsky CR, DeBlieux PMC, Mattu A, Swadron SP, Winters ME. eds. Roberts and Hedges’ Clinical Procedures in Emergency Medicine and Acute Care, 7e. Elsevier; 2019. Accessed July 28, 2022. https://www.clinicalkey.com/#!/content/book/3-s2.0-B9780323354783000555?indexOverride=GLOBAL
Boswell B and Thomas AA. Pediatric Genitourinary and Renal Tract Disorders. In: Walls RM, Hockberger RS, Gausche-Hill M, Erickson TB, Wilcox SR. eds. Rosen’s Emergency Medicine: Concepts and Clinical Practice, 10e. Elsevier; 2023. Accessed July 28, 2022. https://www.clinicalkey.com/#!/content/book/3-s2.0-B9780323757898001687
Davis JE. Male Genital Problems. In: Tintinalli JE, Ma O, Yealy DM, Meckler GD, Stapczynski J, Cline DM, Thomas SH. eds. Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 9e. McGraw Hill; 2020. Accessed July 28, 2022. https://accessmedicine.mhmedical.com/content.aspx?bookid=2353§ionid=219643185
Deveci S. Priapism. In: O’Leary MP and Hockberger RS. eds. UpToDate. Waltham, MA. Accessed July 28, 2022. https://www.uptodate.com/contents/priapism?search=priapism&source=search_result&selectedTitle=1~61&usage_type=default&display_rank=1#H16
RESOURCE AUTHOR(S)
DISCLAIMER
The purpose of this document is to provide health care professionals with key facts and recommendations for the diagnosis and treatment of patients in the emergency department. This summary was produced by Emergency Care BC (formerly the BC Emergency Medicine Network) and uses the best available knowledge at the time of publication. However, healthcare professionals should continue to use their own judgment and take into consideration context, resources and other relevant factors. Emergency Care BC is not liable for any damages, claims, liabilities, costs or obligations arising from the use of this document including loss or damages arising from any claims made by a third party. Emergency Care BC also assumes no responsibility or liability for changes made to this document without its consent.
Last Updated Aug 22, 2022
Visit our website at https://emergencycarebc.ca
COMMENTS (0)
Add public comment…
POST COMMENT
We welcome your contribution! If you are a member, log in here. If not, you can still submit a comment but we just need some information.